Fill a Valid C 08 B Georgia Template
Forms Georgia
Fill a Valid C 08 B Georgia Template
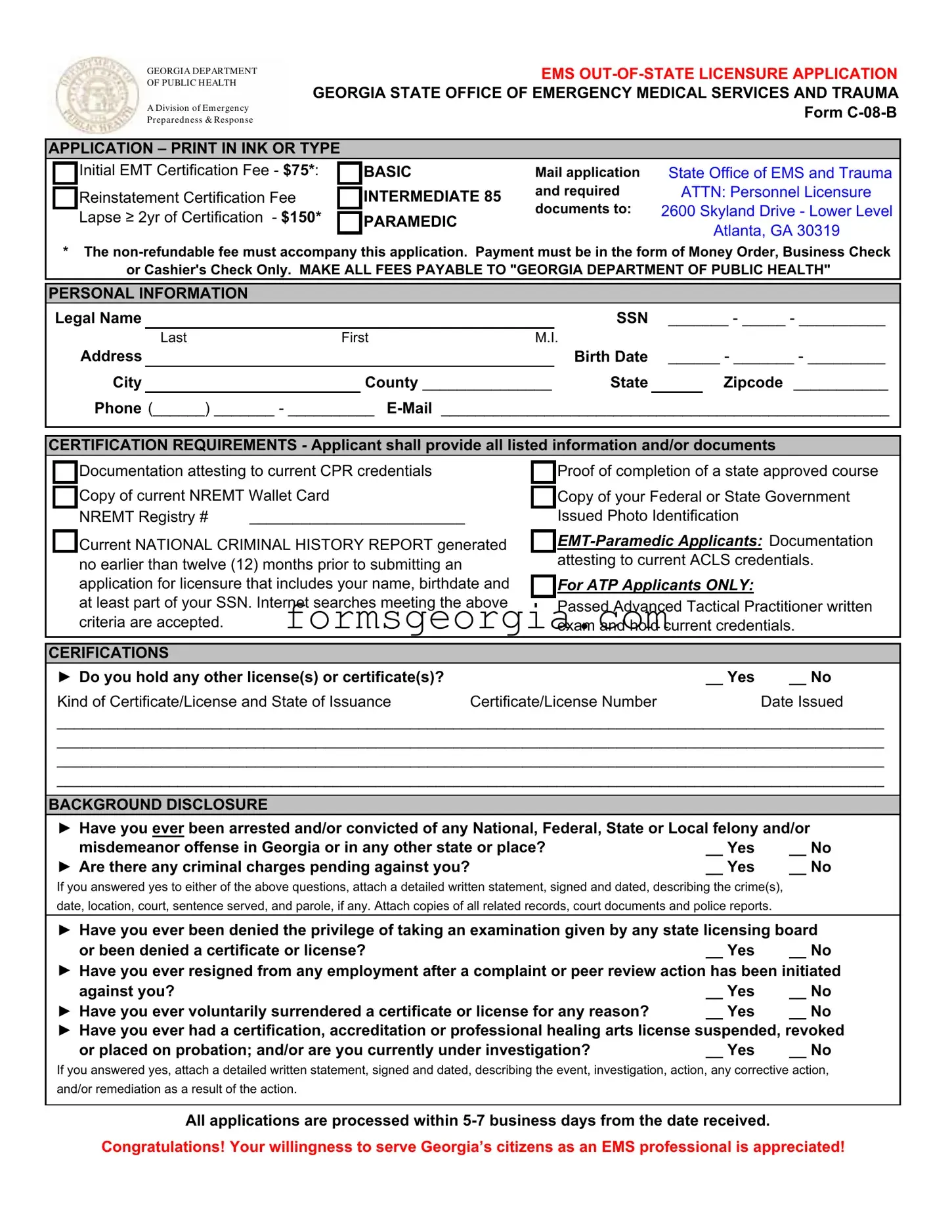
The C 08 B Georgia form serves as a critical tool for individuals seeking out-of-state licensure as Emergency Medical Technicians (EMTs) or paramedics in Georgia. This application is administered by the Georgia Department of Public Health, specifically through the Office of Emergency Medical Services and Trauma. Applicants must provide personal information, including their legal name, Social Security number, and contact details. The form outlines various certification requirements, necessitating documentation such as CPR credentials, proof of course completion, and a National Criminal History Report. Additionally, it addresses background disclosures, requiring applicants to disclose any past arrests, convictions, or disciplinary actions related to licensure. A non-refundable fee accompanies the application, which varies based on the level of certification sought—Basic, Intermediate, or Paramedic. The processing time for applications typically ranges from five to seven business days, emphasizing the importance of thorough and accurate submissions. Completing this form not only reflects an applicant's commitment to serving Georgia's citizens but also ensures compliance with state regulations governing emergency medical services.
GEORGIA DEPARTMENT OF PUBLIC H EALTH
A Division of Em er gen cy Pr epar edn ess & Respon se
EMS
APPLICATION – PRINT IN INK OR TYPE
|
Initial EMT Certification Fee - $75*: |
|
BASIC |
Mail application |
State Office of EMS and Trauma |
|
Reinstatement Certification Fee |
|
INTERMEDIATE 85 |
and required |
ATTN: Personnel Licensure |
|
|
||||
|
|
documents to: |
2600 Skyland Drive - Lower Level |
||
|
Lapse ≥ 2yr of Certification - $150* |
|
PARAMEDIC |
||
|
|
||||
|
|
|
Atlanta, GA 30319 |
||
|
|
|
|
|
* The
or Cashier's Check Only. MAKE ALL FEES PAYABLE TO "GEORGIA DEPARTMENT OF PUBLIC HEALTH"
PERSONAL INFORMATION
Legal Name |
|
|
|
|
|
SSN _______ - _____ - __________ |
||
|
Last |
First |
M.I. |
|
|
|
||
Address |
|
|
|
|
|
Birth Date |
______ - _______ - _________ |
|
City |
|
|
County _______________ |
State |
|
Zipcode ___________ |
||
Phone (______) _______ - __________
CERTIFICATION REQUIREMENTS - Applicant shall provide all listed information and/or documents
|
|
Documentation attesting to current CPR credentials |
|
|
Proof of completion of a state approved course |
||
|
|
Copy of current NREMT Wallet Card |
|
|
Copy of your Federal or State Government |
||
|
|
|
|
||||
|
|
NREMT Registry # |
_________________________ |
|
|
Issued Photo Identification |
|
|
|
Current NATIONAL CRIMINAL HISTORY REPORT generated |
|
||||
|
|
|
|||||
|
|
no earlier than twelve (12) months prior to submitting an |
|
|
attesting to current ACLS credentials. |
||
|
|
|
|
|
|
||
|
|
application for licensure that includes your name, birthdate and |
|
For ATP Applicants ONLY: |
|
||
|
|
at least part of your SSN. Internet searches meeting the above |
|
Passed Advanced Tactical Practitioner written |
|||
|
|
|
|
|
|
||
|
|
criteria are accepted. |
|
|
|
exam and hold current credentials. |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
CERIFICATIONS |
|
|
|
|
|
||
|
► Do you hold any other license(s) or certificate(s)? |
|
|
__ Yes |
__ No |
||
|
Kind of Certificate/License and State of Issuance |
Certificate/License Number |
Date Issued |
||||
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
BACKGROUND DISCLOSURE
► Have you ever been arrested and/or convicted of any National, Federal, State or Local felony and/or
misdemeanor offense in Georgia or in any other state or place? |
__ Yes |
__ No |
► Are there any criminal charges pending against you? |
__ Yes |
__ No |
If you answered yes to either of the above questions, attach a detailed written statement, signed and dated, describing the crime(s), date, location, court, sentence served, and parole, if any. Attach copies of all related records, court documents and police reports.
► Have you ever been denied the privilege of taking an examination given by any state licensing board
or been denied a certificate or license?__ Yes __ No ► Have you ever resigned from any employment after a complaint or peer review action has been initiated
against you? |
__ Yes |
__ No |
► Have you ever voluntarily surrendered a certificate or license for any reason? |
__ Yes |
__ No |
► Have you ever had a certification, accreditation or professional healing arts license suspended, revoked
or placed on probation; and/or are you currently under investigation?__ Yes __ No
If you answered yes, attach a detailed written statement, signed and dated, describing the event, investigation, action, any corrective action, and/or remediation as a result of the action.
All applications are processed within

GEORGIA DEPARTMENT OF PUBLIC H EALTH
A Division of Em er gen cy Pr epar edn ess & Respon se
GEORGIA OFFICE OF EMERGENCY MEDICAL SERVICES AND TRAUMA
AFFIDAVIT OF APPLICANT
I acknowledge and state that I have read and answered all questions in compliance with this application. I acknowledge that it is my responsibility to read and become familiar with the Georgia Department of Public Health Rules and Regulations for Emergency Medical Services
I further state that by filing this application for a license in the State of Georgia, I hereby authorize and consent to have an investigation made as to my moral character, professional reputation and fitness for practice as an EMS provider. I agree to give any further information which may be required in reference to my past record. I understand that I will not receive a copy of the report or know its contents and I further understand that the content of the investigative report will be privileged, unless determined otherwise by the Board or Court Order.
I hereby release, discharge, and exonerate the Georgia Department of Public Health, its agents, representatives, and any person so furnishing information, from any and all liability of every nature and kind arise out of the furnishing or inspection of such documents, records or other information or the investigation made by the Georgia Department of Public Health. I authorize the Georgia Department of Public Health to release information, material, documents, orders of the like relating to me or to this application to any other agency of the State of Georgia, the licensing agency of any other State or Territory of the United States or Province of Canada, a law enforcement agency, a hospital, or other agencies determined by the Board.
This is to certify that the foregoing information is true and correct to the best of my knowledge. I understand that any person who shall give false or forged evidence of any kind to the Board may be prosecuted to the fullest extent allowed by law.
Signature of Applicant |
|
Date |
|
|
|
|
|
Name Of Applicant |
|
City |
State |
Being duly sworn, says that he/she is the person who executed this application for licensure as an EMS provider in the State of Georgia; and that all the statements herein contained are true in every respect and that the attached photo is a true photo of applicant.
Sworn to and subscribed before me this ______ day of ___________, 20_____.
____________________________________________________
Notary Public
My Commission Expires _______________________________
(SEAL)
Attach Photo Here
Notary: DO NOT notarize this section unless a passport photograph is attached.
FORM
GEORGIA DEPARTMENT OF PUBLIC H EALTH
A Division of Em er gen cy Pr epar edn ess & Respon se
GEORGIA OFFICE OF EMERGENCY MEDICAL SERVICES AND TRAUMA
LICENSE VERIFICATION FORM
This form is used to verify the good standing of EMT or paramedic license or certification applicants who are licensed or certified by another state. Please note that you must submit a separate form for each license and/or certification you hold. Your application cannot be processed without this form.
PART I: Completed by Applicant
Legal Name: _______________________________________________ SSN: ______ - ______ - __________
Current Address: ______________________________________________________________________________
______________________________________________________________________________
►I am requesting Georgia license based on the following current license(s) or certification(s):
___ in the state of __________________ AND by the National Registry of EMTs
Current certification(s) or license(s) in another state or issued by the National Registry of EMTs:
EMT - Basic Certificate |
# ______________ |
Expiration Date |
____________________ |
|
EMT - Intermediate Certificate |
# ______________ |
Expiration Date |
____________________ |
|
Paramedic Certificate |
# |
______________ |
Expiration Date |
____________________ |
Other (specify) ______________________________________ |
|
|
||
Certificate |
# |
______________ |
Expiration Date |
____________________ |
PART II: Completed by the State Certifying Agency
Please assist by verifying that this individual is currently certified and in good standing according to your certification policies.
A. Is the
policy? |
__ Yes |
__ No |
B. Has the above certification(s) or license(s) ever been revoked or suspended? |
__ Yes |
__ No |
If yes, please explain ______________________________________________________________________ |
||
__________________________________________________________________________________________
__________________________________________________________________________________________
C. |
Has the above listed individual ever been convicted of a felony? |
__ Yes |
__ No |
|
If yes, what was the offense? _______________________________________________________________ |
||
|
Date of conviction ______________________ Place of conviction ________________________________ |
||
D. |
Do you know of any reason licensure in Georgia should be denied? |
__ Yes |
__ No |
|
If yes, please explain ______________________________________________________________________ |
||
__________________________________________________________________________________________
Title: _________________________
State: _________________________
Date: _________________________
Application Documents
Application Complete
Government Photo ID
Course Completion
NREMT Card
CPR Credentials
Nat'l Criminal Background
Other Certifications
(ATP, ACLS, ETC)
Application Fee
Type: __ M/O __ C/C __ B/C
CH # ________________________
Date: ____/_____/20______
Amount Recv'd: $ _____________
Recv'd by: __________________
|
Certification Status |
Status: __ Approved __ Denied |
|
Date: |
____/_____/20______ |
License # |
___________________ |
Exp Date: |
____/_____/20______ |
Notes: ____________________________
___________________________________
___________________________________
| Fact Name | Fact Description |
|---|---|
| Form Purpose | The C-08-B form is used for out-of-state licensure applications for Emergency Medical Technicians (EMTs) in Georgia. |
| Application Fees | Initial certification fees are $75 for Basic, $85 for Intermediate, and $150 for Paramedic. These fees are non-refundable. |
| Submission Method | Applicants must mail the completed form along with required documents to the Georgia State Office of EMS and Trauma. |
| Required Documents | Applicants must provide proof of CPR credentials, NREMT wallet card, and a national criminal history report, among other documents. |
| Background Disclosure | Applicants must disclose any arrests, convictions, or pending criminal charges, and provide detailed written statements if applicable. |
| Processing Time | All applications are processed within 5-7 business days from the date they are received. |
| Governing Law | This form is governed by the Georgia Department of Public Health Rules and Regulations for Emergency Medical Services (Rule 111-9-2). |
| Notarization Requirement | A notary public must notarize the application, but only if a passport photograph is attached. |
| License Verification | The form includes a section for state certifying agencies to verify the applicant's current license status and any disciplinary actions. |
Form It-303 - For extensions beyond six months, a new IT-303 form and a copy of the first request must be submitted.
The Florida Notary Acknowledgement form is crucial for verifying the identities of individuals signing significant documents. This form, known as a vital resource for any official transaction, emphasizes the importance of understanding one's commitments. For more information, check out this extensive guide on the notary acknowledgement process in Florida.
Georgia 3907 - Ultimately, it represents a convergence of personal history and legal procedure, encapsulating a key moment of change within the formal legal record.