Fill a Valid Georgia Department Of Labor Template
Forms Georgia
Fill a Valid Georgia Department Of Labor Template
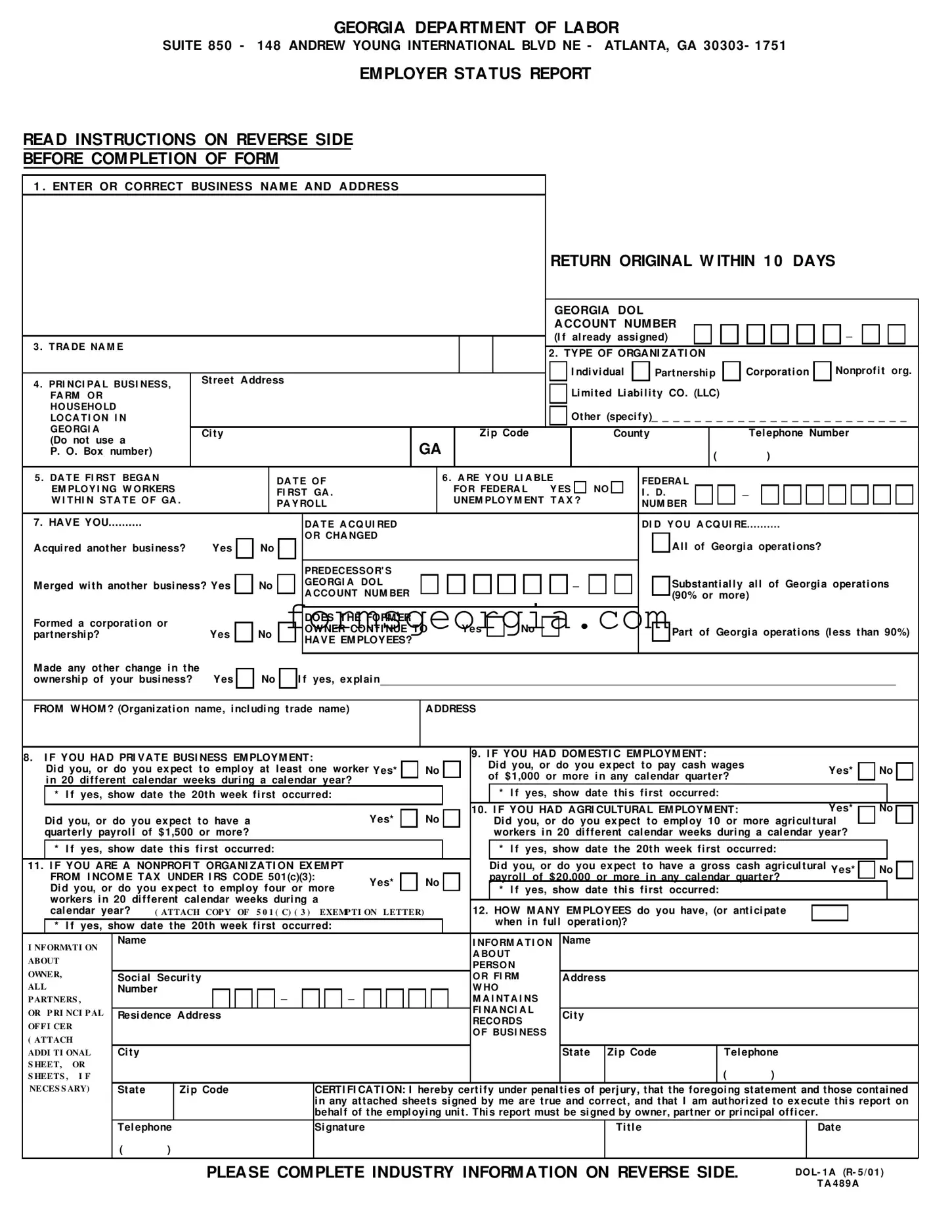
The Georgia Department of Labor form, known as the Employer Status Report, plays a crucial role for businesses operating within the state. This form must be completed accurately and returned within ten days of receipt. It requires employers to provide essential information, including their business name, address, and type of organization, whether it be a corporation, partnership, or nonprofit. Employers must also disclose their Georgia Department of Labor account number, if assigned, and the physical location of their business. The form prompts employers to answer questions about their workforce, including the date they began employing workers in Georgia and whether they are liable for federal unemployment tax. Additionally, it addresses any changes in business ownership, such as mergers or acquisitions, and requires details about the previous owner if applicable. Specific sections focus on various types of employment, including private, domestic, and agricultural, ensuring that all employers report their employment status accurately. Finally, the form includes a certification statement that must be signed by an authorized individual, emphasizing the importance of truthful reporting. Completing this form is not just a regulatory requirement; it is essential for compliance with Georgia's employment security laws.
GEORGIA DEPARTM ENT OF LABOR
SUITE 850 - 148 ANDREW YOUNG INTERNATIONAL BLVD NE - ATLANTA, GA 30303- 1751
EM PLOYER STATUS REPORT
READ INSTRUCTIONS ON REVERSE SIDE
BEFORE COM PLETION OF FORM
1 . ENTER OR CORRECT BUSINESS NA M E A ND A DDRESS
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RETURN ORIGINAL W ITHIN 1 0 DAYS |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
GEORGIA DOL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A CCOUNT NUM BER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_ |
|
|
|
|
|
|
|
|
|||||||||||||
3 . T RA DE NA M E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(I f |
al ready |
assi gned) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. TYPE OF ORGA NI ZA TI ON |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I ndi vi dual |
|
|
|
Part nershi p |
|
|
Corporat i on |
|
|
|
Nonprof i t org. |
|
|||||||||||||||||||||||||
4 . PRI NCI PA L BUSI NESS, |
|
St reet |
A ddress |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Li mi t ed Li abi l i t y CO. (LLC) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
FA RM O R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
HO USEHO LD |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ot her (speci f y)_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ |
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
LO CA T I O N I N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
GEO RGI A |
|
Ci t y |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Zi p Code |
|
|
|
Count y |
|
|
|
|
Tel ephone Number |
|
||||||||||||||||||||||||||||||||||||||||
(Do not use a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
GA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
P. O. Box number) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
|
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
5 . DA T E FI RST BEGA N |
|
|
|
|
DA T E O F |
|
6 . A RE Y O U LI A BLE |
|
|
|
|
|
FEDERA L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
EM PLO Y I NG W O RKERS |
|
|
|
|
FI RST GA . |
|
|
FO R FEDERA L Y ES |
|
NO |
|
|
I . D. |
|
|
|
|
_ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
W I T HI N ST A T E O F GA . |
|
|
|
|
PA Y RO LL |
|
|
UNEM PLO Y M ENT T A X ? |
|
|
NUM BER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
7. HA VE YOU |
|
|
|
|
|
|
|
DA T E A CQ UI RED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DI D Y O U A CQ UI RE |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
A cqui red anot her busi ness? |
Yes |
|
No |
|
|
|
O R CHA NGED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A l l of Georgi a operat i ons? |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PREDECESSO R' S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
M erged wi t h anot her busi ness? Yes |
|
No |
|
|
|
GEO RGI A DO L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Subst ant i al l y |
|
al l of Georgi a operat i ons |
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
A CCO UNT NUM BER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(90% or more) |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Formed a corporat i on or |
|
|
|
|
|
|
|
DOES THE FORM ER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
OWNER CONTI NUE TO |
|
|
|
Yes |
|
|
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Part of Georgi a operat i ons (l ess t han 90%) |
|
|||||||||||||||||||||||||||||||||||||
part nershi p? |
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
HA VE EM PLOYEES? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||
M ade any ot her change i n t he |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
ownershi p of your busi ness? |
Yes |
|
No |
|
|
I f yes, ex pl ai n |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM WHOM ? (Organi zat i on name, i ncl udi ng t rade name)
A DDRESS
8. I F YOU HA D PRI VA TE BUSI NESS EM PLOYM ENT: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. I F YOU HA D DOM ESTI C EM PLOYM ENT: |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
Di d you, or do you ex pect t o empl oy at |
l east one worker Yes* |
|
|
|
No |
|
|
Di d you, or do you ex pect t o pay cash wages |
|
|
Yes* |
|
No |
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
of |
$ 1,000 or more |
i n any cal endar quart er? |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
i n 20 |
di f f erent cal endar weeks duri ng a cal endar year? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
* I f |
yes, show |
dat e |
t he 20t h week f i rst |
occurred: |
|
|
|
|
|
|
|
|
|
|
|
|
|
* |
I f |
yes, show dat e t hi s f i rst |
occurred: |
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes* |
|
|
|
|
No |
|
|
|
10. I F YOU HA D A GRI CULTURA L EM PLOYM ENT: |
|
|
Yes* |
|
No |
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
Di d you, or do you ex pect t o have a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Di d you, or do you ex pect t o empl oy 10 or more agri cul t ural |
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
quart erl y payrol l |
of $ 1,500 or more? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
workers i n 20 di f f erent cal endar weeks duri ng a cal endar year? |
|
|
|
|
|
||||||||||||||||||||
|
* I f |
yes, show |
dat e |
t hi s f i rst occurred: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* |
I f |
yes, show dat e t he 20t h week f i rst occurred: |
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
11. I F YOU A RE A NONPROFI T ORGA NI ZA TI ON EX EM PT |
|
|
|
|
|
|
|
|
|
|
|
|
|
Di d you, or do you ex pect t o have a gross cash agri cul t ural Yes* |
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No |
|
|
||||||||||||||||||||||||||||||||
|
FROM I NCOM E TA X |
UNDER I RS CODE 501(c)(3): |
Yes* |
|
|
|
|
No |
|
|
|
|
payrol l of $ 20,000 or more i n any cal endar quart er? |
|
|
|
|
|
||||||||||||||||||||||||||||||
|
Di d you, or do you ex pect t o empl oy f our or more |
|
|
|
|
|
|
|
* |
I f |
yes, show dat e t hi s f i rst |
occurred: |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
workers i n 20 di f f erent cal endar weeks duri ng a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
cal endar year? |
( ATTACH COP Y OF 5 0 1 ( C) ( 3 ) |
|
EXEMP TI ON LETTER) |
|
|
12. HOW M A NY EM PLOYEES do you have, (or ant i ci pat e |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
* I f |
yes, show |
dat e |
t he 20t h week f i rst |
occurred: |
|
|
|
|
|
|
|
|
|
|
|
|
|
when i n f ul l |
operat i on)? |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
I NF ORMATI ON |
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I NFO RM A T I O N |
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A BO UT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
ABOUT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PERSO N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
OWNER, |
|
Soci al Securi t y |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O R FI RM |
|
A ddress |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
ALL |
|
Number |
|
|
|
|
|
|
|
_ |
|
|
|
|
_ |
|
|
|
|
|
|
|
|
|
|
|
|
|
W HO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
P ARTNERS , |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M A I NT A I NS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
OR P RI NCI P AL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FI NA NCI A L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Resi dence A ddress |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ci t y |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RECO RDS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
OF F I CER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O F BUSI NESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
( ATTACH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
ADDI TI ONAL |
Ci t y |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
St at e |
|
Zi p Code |
|
Tel ephone |
|
|
|
|
|
||||||
S HEET, OR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
S HEETS , |
I F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
NECES S ARY) |
St at e |
|
Zi p Code |
|
|
CERTI FI CA TI ON: I |
hereby cert i f y under penal t i es of perj ury, t hat t he f oregoi ng st at ement and t hose cont ai ned |
|
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
i n any at t ached sheet s si gned by me are t rue and correct , and t hat I am aut hori zed t o ex ecut e t hi s report on |
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
behal f of t he empl oyi ng uni t . Thi s report must be si gned by owner, part ner or pri nci pal of f i cer. |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
Tel ephone |
|
|
Si gnat ure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ti t l e |
|
|
|
|
Dat e |
|
|
|
|
|
|||||||||||||
|
|
|
( |
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLEASE COM PLETE INDUSTRY INFORM ATION ON REVERSE SIDE.
DO L- 1 A (R- 5 / 0 1 )
T A 4 8 9 A
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(CONTINUED) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
NATURE OF BUSINESS: Inf ormation |
is |
required on all items. Attach additional sheets, |
if |
necessary. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
A . How many Georgia locations do |
you operate? |
|
|
|
|
|
|
C. Enter in order of importance and indicate |
|||||||||||||||||||||||||||||
|
Provide |
the |
f ollow ing |
inf ormation |
f or |
each location, |
attaching |
additional |
|
|
|
approximate % of total annual income derived |
|||||||||||||||||||||||||
|
sheets |
if |
necessary. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
f rom each: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
B. Check the box that best |
describes |
the industry |
that |
relates |
to |
your |
|
|
|
Principal |
Service(s) |
OR |
|
Principal Product(s) |
|||||||||||||||||||||||
|
business |
activities: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rendered* |
|
|
|
Mf g. |
Grow n |
Sold |
||||||||||||||
|
|
|
|
|
|
|
|
|
Manuf acturing |
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
Agriculture |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
% |
||||||||
|
Forestry |
|
|
|
|
|
|
|
|
|
|
Transportation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
% |
||||||
|
|
|
|
|
|
|
|
|
|
|
Communication |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Fishing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
% |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
Public |
Utilities |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Mining |
|
|
|
|
|
|
|
|
|
|
|
|
|
* |
I f |
Transport at i on- Trucki ng, |
i ndi cat e |
i f i nt erst at e carri er |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
W holesale Trade |
|
|||||||||||||||||||||||
|
Construction (specif y): |
|
|
|
|
|
|
|
|
D. If |
this report includes |
establishment(s) |
that |
only |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
Retail |
Trade |
|
|||||||||||||||||||||||||||
|
General |
Contractors |
Industrial_ |
_ |
_ |
% |
|
|
|
|
|
perf orm |
services |
f or other units of |
the |
company, |
|||||||||||||||||||||
|
|
|
Finance |
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
indicate |
the primary type of |
|
service or support |
|||||||||||||||
|
Residential_ |
_ |
_ % Commercial_ |
_ |
_ |
% |
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
Insurance |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
Speculative |
Building |
|
|
|
|
|
|
|
|
|
|
|
|
provided. |
Check |
as many as apply: |
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
Real Estate |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Special |
Trade |
Contractor |
(specif y plumbing, |
|
|
|
1 . |
|
Central |
Administration |
3 . |
Storage (w arehouse) |
||||||||||||||||||||||||
|
|
|
Services |
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
etc.,)_ |
_ _ |
_ |
_ _ _ _ |
_ |
_ _ _ |
_ |
_ |
_ |
_ _ |
|
|
|
|
2 . |
|
Research,development, |
4 . |
Other: (specif y), |
||||||||||||||||||
|
|
|
Public |
Administration |
|
|
|||||||||||||||||||||||||||||||
|
Heavy Construction (specif y cable, |
highw ay, |
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
Private |
Household |
|
|
|
|
and |
testing |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
etc.,)_ |
_ |
_ _ |
_ _ _ _ |
_ |
_ _ _ _ _ |
_ |
_ _ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
Employer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR ASSISTANCE, |
call |
the Industry Classif ication |
Unit, |
(4 0 4 ) 6 5 6 - 3 1 7 7 |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IMPORTANT - This report must be f iled! The law provides that all employing units shall f ile a report of its employment during a calendar year. For the purpose of aiding you in complying w ith OCGA Section 3 4 - 8 - 1 2 1 of the Employment Security Law , this f orm has been prepared to assist you in f urnishing the required inf ormation. Answ er all questions f ully and if additional space is necessary under any item, attach signed and dated sheets w hich bear the w ords "Supplement to Form DOL- 1 ."
Each f alse statement or w illf ul f ailure to f urnish this report is punishable as a crime. Each day of such f ailure or ef usal constitutes a separate of f ense.
The Georgia Employer Status Report is required of all employers having individuals perf orming services in Georgia regardless of number or duration of time.
The f iling of this f orm is required at the time your business f irst had individuals perf orming service in Georgia, or w hen you acquired another legal entity, and may also be required again upon request.
NOTE: Disclosure of your social security number is mandatory. It will be used f or the purpose of identif ication and it is required under the authority of 42 U.S.C. Section405(2)(c)andOCGASection 34- 8- 121(a).
IN S TRUCTIO N S
(NUMBERS CORRESPOND TO ITEMS ON FORM)
1 . Enter or correct name and address of individual ow ner, partners, corporation or organization. This is the address to w hich you authorize us to mail all reports, correspondence, etc. If you have already been assigned a Georgia Department of Labor Account Number (Ga. DOL Acct. No) by this Department, please insert the number.
2 . Indicate by check mark type of organization. If a nonprof it organization, attach copy of I.R.S. letter ex empting the organization f rom Federal Income Tax under Section 5 0 1 (c)(3 ) of Internal Revenue Code.
3 . Trade name by w hich business is know n if dif f erent than 1 .
4 . Physical location of business, f arm or household in Georgia if dif f erent than 1 . Please include telephone number w ith area code.
5 . Enter the f irst date of employment in Georgia and the f irst date of Georgia payroll.
6 . If you are subj ect to the Federal Unemployment Tax Act, and are required to f ile Federal Form 9 4 0 , answ er this question "yes". Be sure to enter your Federal Employer Identif ication Number w hether answ ered "yes" or "no".
7 . Answ er this question if you acquired this business f rom another employer or if af ter you began employing w orkers you have acquired other businesses; merged w ith other businesses; f ormed or dissolved partnerships, corporations, prof essional associations; or if any other change in the ow nership of the business has occurred. Indicate the date of acquisition or change and provide all inf ormation concerning the previous ow ner's name, trade name, address and DOL Account Number. Indicate by checking the appropriate block the portion of the previous ow ner's business involved in the acquisition or change. No transf er of ex perience rating history can be made unless inf ormation concerning the previous ow ner is provided.
8 . Private Business Employment - Most employment is considered private business employment. This includes all types of w ork ex cept domestic service such as maids, gardeners, cooks, etc., agricultural service and service perf ormed f or governmental or nonprof it organizations.
9 . Domestic employment includes all service f or a person in the operation and maintenance of a private household, local college club or local chapter of a college f raternity or sorority such as chauf f eurs, cooks, babysitters, gardeners, maids, butlers, private and/ or social secretaries, etc. If you had such employment, consider only cash payments made to all individuals perf orming domestic services to determine if $1 ,0 0 0 or more cash w ages w ere paid in any calendar quarter during 1 9 7 7 and subsequent quarters.
1 0 |
. Consider only cash payments made to all individuals perf orming agricultural services to determine if $2 0 ,0 0 0 or more cash w ages w ere paid in |
|||
|
any calendar quarter during 1 9 7 7 and subsequent quarters. |
|
||
1 1 |
. Answ er this question only if this business is a nonprof it organization ex empt f rom Federal Income Tax under Section 5 0 1 (c)(3 ) of the Internal |
|||
|
Revenue Code. Attach a copy of the I.R.S. letter granting this ex emption. Nonprof it organizations w ith tax ex emptions other than under Section |
|||
|
5 0 1 (c)(3 ) should answ er question 8 , Private Business Employment. |
|
||
1 2 |
. Self - ex planatory. |
|
|
|
|
|
|
|
|
|
|
FOR ASSISTANCE, call the Adj udication Section, (4 0 4 ) 6 5 6 - 3 0 6 9 |
|
|
Please RETAIN a copy f or your |
f iles. |
RETURN ORIGINAL WITHIN TEN (10) DAYS TO: |
Georgia Department of Labor |
|
|
|
|
|
P O Box 7 4 0 2 3 4 |
The |
enclosed envelope requires |
postage. |
|
Atlanta, GA 3 0 3 7 4 - 0 2 3 4 |
|
|
|||
| Fact Name | Details |
|---|---|
| Purpose of the Form | The Georgia Department of Labor Form is used to report employer status and employment information for businesses operating in Georgia. |
| Submission Deadline | Employers must return the original form within 10 days of completion to comply with state regulations. |
| Governing Law | This form is governed by the Georgia Employment Security Law, specifically OCGA Section 34-8-121. |
| Required Information | Employers must provide their business name, address, type of organization, and Georgia DOL account number if applicable. |
| Liability for Taxes | The form asks if the employer is liable for federal unemployment tax, which is crucial for tax compliance. |
| Nonprofit Organizations | Nonprofits must attach a copy of their IRS exemption letter under Section 501(c)(3) to the form. |
| Employment Types | Employers must indicate whether they have private, domestic, or agricultural employment, as these categories have different reporting requirements. |
| Penalties for Noncompliance | Failure to file this report accurately or timely may result in penalties, including fines for false statements. |
Georgia Form 700 Instructions 2023 - Subtractions for items such as interest on U.S. obligations are available on this tax return.
The Florida Real Estate Purchase Agreement is a critical document for anyone venturing into property transactions. For detailed information on this process, you can refer to this resource: a thorough guide on the Real Estate Purchase Agreement, which outlines important aspects and requirements to ensure a smooth transaction.
Georgia Net Worth Tax - Assists in the prevention of fraud by requiring detailed documentation and certification of preneed contract funds.