Fill a Valid Georgia Medicaid Application Template
Forms Georgia
Fill a Valid Georgia Medicaid Application Template
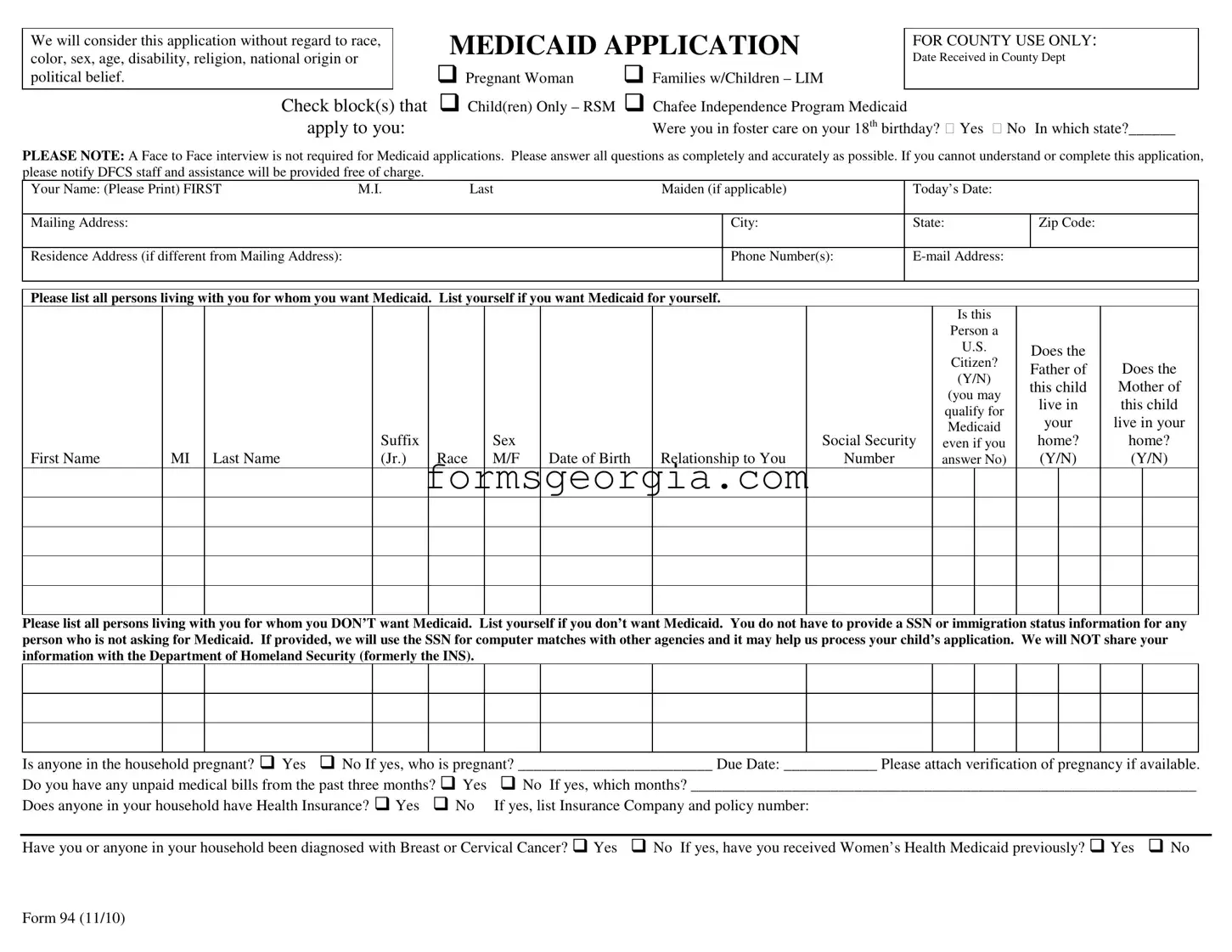
Navigating the Georgia Medicaid application form can feel overwhelming, but understanding its key components can make the process smoother. This form is designed to assess eligibility for various Medicaid programs, including those for pregnant women, families with children, and individuals who were in foster care. It requires applicants to provide personal information such as their name, address, and contact details, as well as details about household members seeking coverage. You will need to indicate your citizenship status, provide information about any health insurance you may have, and disclose income sources. The form also includes sections for reporting any unpaid medical bills and for detailing dependent care expenses. Importantly, applicants are encouraged to complete the form as accurately as possible, as this will help expedite the review process. Assistance is available for those who need help filling it out. Remember, a face-to-face interview is not required, so you can submit your application conveniently. By taking the time to understand these aspects, you can approach the application process with confidence.
We will consider this application without regard to race, color, sex, age, disability, religion, national origin or political belief.
Check block(s) that apply to you:
MEDICAID APPLICATION |
FOR COUNTY USE ONLY: |
|
Date Received in County Dept |
||
|
Pregnant Woman Families w/Children – LIM
Child(ren) Only – RSM Chafee Independence Program Medicaid
Were you in foster care on your 18th birthday? Yes No In which state?______
PLEASE NOTE: A Face to Face interview is not required for Medicaid applications. Please answer all questions as completely and accurately as possible. If you cannot understand or complete this application, please notify DFCS staff and assistance will be provided free of charge.
Your Name: (Please Print) FIRST |
M.I. |
|
Last |
|
Maiden (if applicable) |
|
Today’s Date: |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address: |
|
|
|
|
|
|
|
|
|
City: |
|
State: |
|
Zip Code: |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Residence Address (if different from Mailing Address): |
|
|
|
|
|
|
|
Phone Number(s): |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Please list all persons living with you for whom you want Medicaid. List yourself if you want Medicaid for yourself. |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Is this |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Person a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
U.S. |
|
Does the |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Citizen? |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Father of |
Does the |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
(Y/N) |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
this child |
Mother of |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
(you may |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
live in |
this child |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
qualify for |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
your |
live in your |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Medicaid |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Suffix |
|
|
Sex |
|
|
|
Social Security |
even if you |
|
home? |
home? |
||||
First Name |
MI |
Last Name |
|
(Jr.) |
Race |
|
M/F |
Date of Birth |
Relationship to You |
Number |
|
answer No) |
|
(Y/N) |
(Y/N) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please list all persons living with you for whom you DON’T want Medicaid. List yourself if you don’t want Medicaid. You do not have to provide a SSN or immigration status information for any person who is not asking for Medicaid. If provided, we will use the SSN for computer matches with other agencies and it may help us process your child’s application. We will NOT share your information with the Department of Homeland Security (formerly the INS).
Is anyone in the household pregnant? Yes No If yes, who is pregnant? _________________________ Due Date: ____________ Please attach verification of pregnancy if available.
Do you have any unpaid medical bills from the past three months? Yes |
No If yes, which months? _________________________________________________________________ |
Does anyone in your household have Health Insurance? Yes No |
If yes, list Insurance Company and policy number: |
Have you or anyone in your household been diagnosed with Breast or Cervical Cancer? Yes No If yes, have you received Women’s Health Medicaid previously? Yes No
Form 94 (11/10)

INCOME, RESOURCES and DAYCARE
List all income received by persons on page 1 of this application. Be sure to show the amount before deductions. Attach an extra sheet if necessary. We will decide, based on the type of Medicaid, whose income must be counted and whose may be excluded. If you are applying for Children Only or Pregnant Woman Medicaid, you do not have to complete the Resources/Vehicles sections below.
|
Gross Amount per Pay |
How Often? |
|
|
|
|
|
|
Amount in |
|
Who Owns |
||
|
Check |
(weekly, every |
|
|
|
|
|
|
|
||||
Income |
(amount before deductions) |
monthly, etc.?) |
Name of Person Receiving |
|
Resources |
|
Account/Value |
|
Resource? |
||||
Wages/Earnings |
|
|
|
|
Cash |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Current Employer: |
|
|
|
|
Checking Account |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Wages/Earnings |
|
|
|
|
Savings Account |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Current Employer: |
|
|
|
|
Credit Union |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Social Security |
|
|
|
|
401K/Retirement |
|
|
|
|
|
|
|
|
Income/SSI |
|
|
|
|
Account |
|
|
|
|
|
|
|
|
Worker’s |
|
|
|
|
|
|
|
|
|
|
|
|
|
Compensation |
|
|
|
|
Other |
|
|
|
|
|
|
|
|
Pensions or |
|
|
|
|
Vehicle(s): Cars, trucks, motorcycles (licensed) |
||||||||
Retirement Benefits |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Child Support/ |
|
|
|
|
Make |
|
Model |
|
Year |
|
Amount |
||
Contributions |
|
|
|
|
|
|
|
Owed? |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||
Unemployment |
|
|
|
|
|
|
|
|
|
|
|
|
|
Benefits |
|
|
|
|
|
|
|
|
|
|
|
|
|
Other Income, please |
|
|
|
|
|
|
|
|
|
|
|
|
|
specify: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Do you pay for dependent care (daycare for a child or care for an adult who cannot care for himself/herself) so that someone in your household can work?
Name of Parent who works
Name of child or adult cared for
Name of care provider
Amount of Payment
How Often? (weekly,
monthly, etc)
If you are applying for Medicaid for children and one or both of their parents are not in the home, please provide the following information:
Child’s Name
Absent Parent’s Name (Mother/Father)
Do they have Medical Coverage on the Child?
Yes/No
If Yes to Medical Coverage, please list name
of insurance company & group number
I understand that this information may need to be verified to determine eligibility. I understand wage and salary information supplied by the Georgia Department of Labor may be obtained to verify and determine eligibility for Medicaid. I agree to assign to the state all rights to medical support and third party support payments (hospital and medical benefits). I agree to give the State the right to require an absent parent provide medical insurance, if available. I understand I must get medical support from the absent parent if it is available and must cooperate with the Division of Child Support Services in obtaining this support. If I do not cooperate, I understand I may lose my Medicaid benefits, and only my children will receive benefits unless good cause is established. I understand that I must report changes in my income and circumstances within ten (10) days of becoming aware of the change.
I certify under penalty of perjury that I am a U.S. Citizen and/or lawfully present in the United States. If I am a parent or legal guardian, I certify that the applicant(s) is a U.S. Citizen
and/or lawfully present in the United States. I certify to the best of my knowledge and belief that the person(s) for whom I am applying for Medicaid is/are U.S. citizen(s) or are lawfully present in the United States. I further certify that all of the information provided on this application is true and correct to the best of my knowledge.
Signature (Required): ______________________________________________________________________________ |
Date: ______________________________ |
Form 94 (11/10)
| Fact Name | Description |
|---|---|
| Non-Discrimination Policy | The Georgia Medicaid Application form states that the application will be considered without regard to race, color, sex, age, disability, religion, national origin, or political belief. |
| Interview Requirement | A face-to-face interview is not required for Medicaid applications. Applicants can complete the form without an in-person meeting. |
| Eligibility Verification | Applicants must provide accurate information. The Georgia Department of Labor may verify wage and salary information to determine eligibility. |
| Governing Law | The Georgia Medicaid program operates under Title XIX of the Social Security Act and state regulations governing Medicaid eligibility. |
G-7 Return - Utilizing the Georgia G-7 form helps employers maintain good standing with state tax authorities by demonstrating diligence in tax reporting.
Employers considering a legal framework to safeguard their business interests might find the significance of a robust Non-compete Agreement essential during employee transitions. For further details, refer to this critical Non-compete Agreement form which outlines the important terms and conditions. Understanding how this form functions can help in navigating competitive landscapes effectively.
Uncontested Divorce in Georgia - Disclose any prior custody actions involving minor children, critical for court consideration in your current divorce petition.
Georgia Workers Compensation - By filling out the WC-200a, employees can smoothly transition to a new treating physician without hindrance to their workers' compensation benefits.