Fill a Valid Georgia Wc 102B Template
Forms Georgia
Fill a Valid Georgia Wc 102B Template
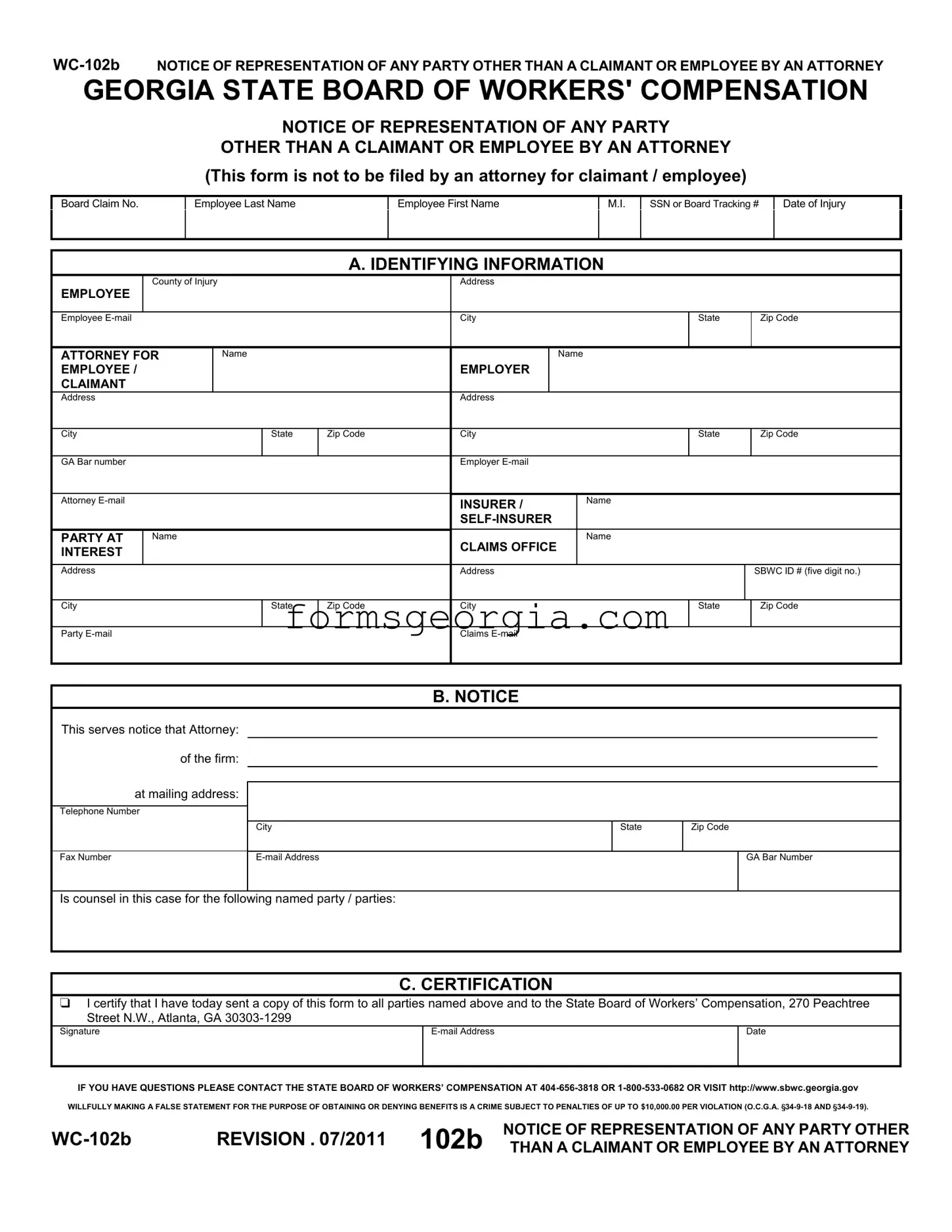
The Georgia WC 102B form plays a critical role in the workers' compensation process, specifically when an attorney represents a party other than the claimant or employee. This form is essential for ensuring that all parties involved in a workers' compensation case are properly notified of legal representation. It captures vital information, including the names and contact details of the employee, employer, and attorney, along with the specifics of the case such as the Board Claim Number and date of injury. The form requires the attorney to certify that a copy has been sent to all relevant parties and the Georgia State Board of Workers' Compensation, which is crucial for maintaining transparency and accountability in the legal process. By providing clear identification of the parties involved, the WC 102B helps to streamline communication and fosters a more organized approach to handling workers' compensation claims. Furthermore, it underscores the importance of accurate documentation in legal proceedings, as any false statements made on this form can lead to significant penalties. Understanding the nuances of this form is essential for anyone navigating the complexities of workers' compensation in Georgia.
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
NOTICE OF REPRESENTATION OF ANY PARTY
OTHER THAN A CLAIMANT OR EMPLOYEE BY AN ATTORNEY
(This form is not to be filed by an attorney for claimant / employee)
Board Claim No.
Employee Last Name
Employee First Name
M.I.
SSN or Board Tracking #
Date of Injury
A. IDENTIFYING INFORMATION
County of Injury
EMPLOYEE
Employee
Address
City
State
Zip Code
ATTORNEY FOR EMPLOYEE / CLAIMANT
Name
EMPLOYER
Name
|
Address |
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
Zip Code |
City |
|
State |
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
GA Bar number |
|
|
|
|
Employer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Attorney |
|
|
|
|
INSURER / |
Name |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PARTY AT |
Name |
|
|
CLAIMS OFFICE |
Name |
|
|||
|
INTEREST |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
Address |
|
|
|
SBWC ID # (five digit no.) |
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
Zip Code |
City |
|
State |
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
Party
Claims
B. NOTICE
This serves notice that Attorney: |
|
|
|
of the firm: |
|
|
|
at mailing address: |
|
|
|
Telephone Number |
|
|
|
|
City |
State |
Zip Code |
Fax Number |
|
GA Bar Number |
Is counsel in this case for the following named party / parties:
C. CERTIFICATION
 I certify that I have today sent a copy of this form to all parties named above and to the State Board of Workers’ Compensation, 270 Peachtree Street N.W., Atlanta, GA
I certify that I have today sent a copy of this form to all parties named above and to the State Board of Workers’ Compensation, 270 Peachtree Street N.W., Atlanta, GA
Signature |
Date |
|
|
|
|
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
REVISION . 07/2011 102b |
NOTICE OF REPRESENTATION OF ANY PARTY OTHER |
|
THAN A CLAIMANT OR EMPLOYEE BY AN ATTORNEY |
| Fact Name | Fact Description |
|---|---|
| Form Purpose | The WC-102B form serves as a notice of representation for any party other than a claimant or employee by an attorney. |
| Governing Law | This form is governed by the Georgia Workers' Compensation Act, specifically O.C.G.A. § 34-9-18 and § 34-9-19. |
| Filing Requirement | Attorneys representing claimants or employees do not file this form. |
| Information Required | Essential information includes the employee's name, date of injury, and the attorney's contact details. |
| Certification Statement | The attorney must certify that a copy of the form has been sent to all relevant parties and the State Board of Workers’ Compensation. |
| Submission Address | The form must be sent to the State Board of Workers’ Compensation at 270 Peachtree Street N.W., Atlanta, GA 30303-1299. |
| Contact Information | For questions, individuals can contact the State Board of Workers’ Compensation at 404-656-3818 or 1-800-533-0682. |
| Penalties for False Statements | Submitting false information can lead to penalties up to $10,000 per violation. |
| Revision Date | The WC-102B form was last revised in July 2011. |
Georgia Preliminary Notice of Lien Rights - Designed to strengthen the financial security of subcontractors and suppliers in Georgia by formally announcing their claim to payments on construction projects.
Georgia Workers Compensation - The WC-200a form represents a key mechanism in the administration of Georgia's workers' compensation laws, fostering an environment of cooperation and support for injured workers.