Fill a Valid Georgia Wc 104 Template
Forms Georgia
Fill a Valid Georgia Wc 104 Template
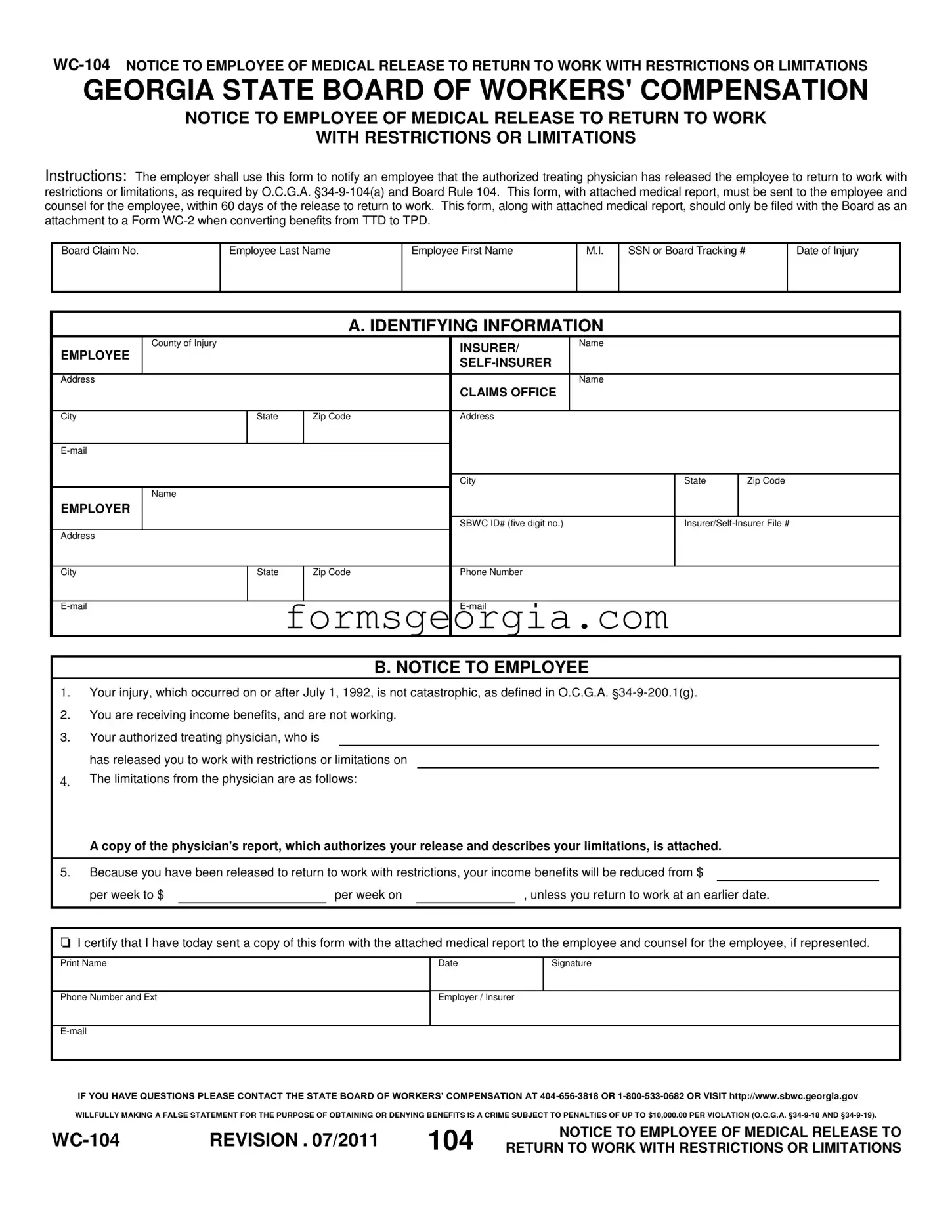
The Georgia WC-104 form serves as a crucial communication tool between employers and employees in the context of workers' compensation. This form is specifically designed to inform employees when their authorized treating physician has cleared them to return to work, albeit with certain restrictions or limitations. It is essential for employers to adhere to the requirements outlined in O.C.G.A. §34-9-104(a) and Board Rule 104 when using this form. Within 60 days of the medical release, employers must send the completed form, along with the physician's medical report, to both the employee and their legal counsel, if applicable. The WC-104 not only provides the necessary details about the employee's injury and the nature of their work restrictions but also outlines the implications for their income benefits. If an employee is released to work with limitations, their weekly benefits may be adjusted accordingly. This form plays a vital role in ensuring that employees are informed about their rights and responsibilities as they transition back to work after an injury.
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
NOTICE TO EMPLOYEE OF MEDICAL RELEASE TO RETURN TO WORK
WITH RESTRICTIONS OR LIMITATIONS
Instructions: The employer shall use this form to notify an employee that the authorized treating physician has released the employee to return to work with restrictions or limitations, as required by O.C.G.A.
Board Claim No.
Employee Last Name
Employee First Name
M.I.
SSN or Board Tracking #
Date of Injury
|
|
|
A. IDENTIFYING INFORMATION |
|
|
||
|
County of Injury |
|
|
INSURER/ |
Name |
|
|
EMPLOYEE |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
Name |
|
|
|
|
|
|
|
CLAIMS OFFICE |
|
|
|
|
|
|
|
|
|
|
|
City |
State |
Zip Code |
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
State |
Zip Code |
|
Name |
|
|
|
|
|
|
EMPLOYER |
|
|
|
|
|
|
|
|
|
|
|
SBWC ID# (five digit no.) |
|
||
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
State |
Zip Code |
Phone Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. NOTICE TO EMPLOYEE
1.Your injury, which occurred on or after July 1, 1992, is not catastrophic, as defined in O.C.G.A.
2.You are receiving income benefits, and are not working.
3.Your authorized treating physician, who is
has released you to work with restrictions or limitations on
4.The limitations from the physician are as follows:
A copy of the physician's report, which authorizes your release and describes your limitations, is attached.
5.Because you have been released to return to work with restrictions, your income benefits will be reduced from $
|
per week to $ |
|
per week on |
|
, unless you return to work at an earlier date. |
|
I certify that I have today sent a copy of this form with the attached medical report to the employee and counsel for the employee, if represented.
Print Name
Date
Signature
Phone Number and Ext
Employer / Insurer
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION . 07/2011 |
104 |
NOTICE TO EMPLOYEE OF MEDICAL RELEASE TO |
|
RETURN TO WORK WITH RESTRICTIONS OR LIMITATIONS |
| Fact Name | Description |
|---|---|
| Purpose of the WC-104 Form | This form is used to notify employees that they have been medically cleared to return to work, albeit with certain restrictions or limitations. |
| Governing Laws | The use of the WC-104 form is mandated by O.C.G.A. §34-9-104(a) and Board Rule 104, which outline the requirements for notifying employees about their return to work status. |
| Submission Timeline | Employers are required to send the WC-104 form to the employee and their counsel within 60 days of the employee's medical release to return to work. |
| Income Benefits Adjustment | Upon release to work with restrictions, the employee's income benefits may be reduced, reflecting their new work status. |
| Attachment Requirement | The WC-104 form must be accompanied by the physician's report detailing the employee's limitations and should be attached to a Form WC-2 when converting benefits. |
| False Statement Penalties | Submitting false information on this form can lead to serious legal consequences, including penalties of up to $10,000, as outlined in O.C.G.A. §34-9-18 and §34-9-19. |
Georgia State Income Tax Forms - Enables a thorough review of the childcare needs and arrangements for foster children, promoting their welfare and development.
Dma-6 Form Pdf - Detailed sections regarding surgeries, therapy visits, neurological status, and more offer a thorough overview of the child’s health needs.
When engaging in a motorcycle transaction in California, it is essential to utilize the California Motorcycle Bill of Sale to ensure a smooth process. This document not only legitimizes the transfer of ownership but also protects both parties involved by documenting the sale details. For those looking for a reliable template, you can find one at https://templates-guide.com/california-motorcycle-bill-of-sale-template/, which simplifies the process of completing this important form.
Ga Workers Compensation - Accuracy in filling out the form aids in establishing the legitimacy of the workers' compensation claim, facilitating a smoother resolution process.