Fill a Valid Georgia Wc 14 Template
Forms Georgia
Fill a Valid Georgia Wc 14 Template
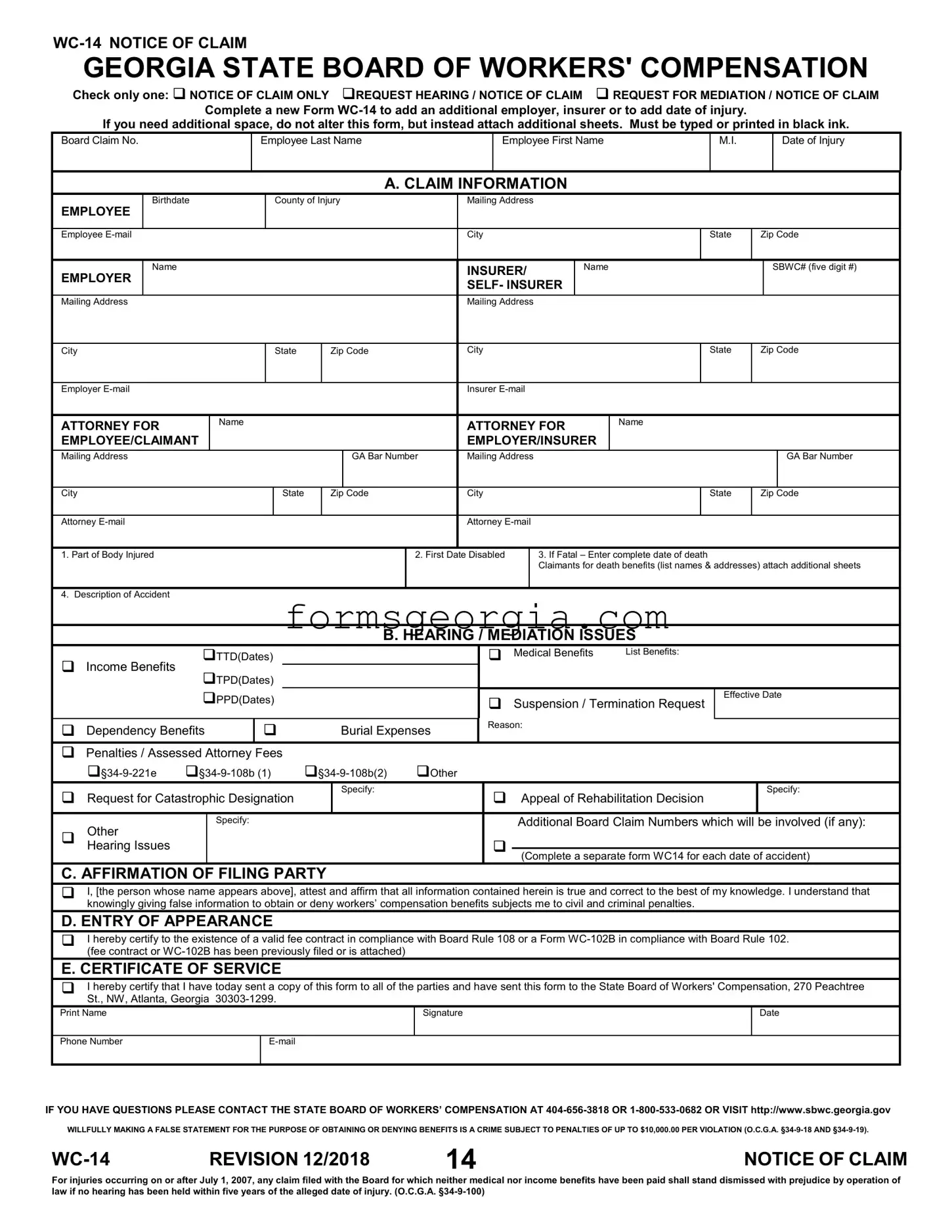
The Georgia WC-14 form plays a crucial role in the workers' compensation process within the state. This form serves as a formal notice of claim, allowing employees to assert their rights when they have suffered injuries on the job. It can be used in various situations, including simply notifying the board of a claim, requesting a hearing, or seeking mediation. When completing the WC-14, individuals must provide essential information such as their name, date of injury, and details about the employer and insurer involved. The form also includes sections to specify the nature of the claim, including medical benefits and income benefits, along with any additional issues related to the case. Importantly, it requires an affirmation of the accuracy of the information provided, ensuring that all parties are held accountable for the details submitted. Furthermore, the WC-14 emphasizes the necessity of compliance with legal requirements, such as filing deadlines and the potential consequences of false statements. By understanding the various components and requirements of the WC-14 form, employees can better navigate the complexities of the workers' compensation system in Georgia.
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
Check only one: NOTICE OF CLAIM ONLY REQUEST HEARING / NOTICE OF CLAIM REQUEST FOR MEDIATION / NOTICE OF CLAIM
Complete a new Form
If you need additional space, do not alter this form, but instead attach additional sheets. Must be typed or printed in black ink.
Board Claim No.
Employee Last Name
Employee First Name
M.I.
Date of Injury
A. CLAIM INFORMATION
EMPLOYEE
Birthdate
County of Injury
Mailing Address
Employee
City
State
Zip Code
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
INSURER/ |
|
Name |
|
|
|
|
|
SBWC# (five digit #) |
||||
EMPLOYER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
SELF- INSURER |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
State |
Zip Code |
City |
|
|
|
|
|
|
State |
Zip Code |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Employer |
|
|
|
|
|
|
|
|
|
Insurer |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ATTORNEY FOR |
|
Name |
|
|
|
ATTORNEY FOR |
Name |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
EMPLOYEE/CLAIMANT |
|
|
|
|
|
|
|
|
|
EMPLOYER/INSURER |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Mailing Address |
|
|
|
|
|
|
|
GA Bar Number |
Mailing Address |
|
|
|
|
|
|
|
|
GA Bar Number |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
City |
|
|
|
|
|
State |
Zip Code |
City |
|
|
|
|
|
|
State |
Zip Code |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Attorney |
|
|
|
|
|
|
|
|
|
Attorney |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
1. Part of Body Injured |
|
|
|
|
|
|
|
|
2. First Date Disabled |
|
|
3. If Fatal – Enter complete date of death |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Claimants for death benefits (list names & addresses) attach additional sheets |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. Description of Accident |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
B. HEARING / MEDIATION ISSUES |
|
|
|
|
|
|||||||||
|
|
TTD(Dates) |
|
|
|
|
|
|
Medical Benefits |
List Benefits: |
|
|
|
|
|
||||||||
Income Benefits |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
TPD(Dates) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
PPD(Dates) |
|
|
|
|
Suspension / Termination Request |
|
Effective Date |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
Reason: |
|
|
|
|
|
|
|
|
|
||
Dependency Benefits |
|
|
Burial Expenses |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Penalties / Assessed Attorney Fees
|
Other |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Request for Catastrophic Designation |
|
Specify: |
|
|
Appeal of Rehabilitation Decision |
Specify: |
||
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Other |
|
Specify: |
|
|
|
|
Additional Board Claim Numbers which will be involved (if any): |
|
|
|
|
|
|
|
|
|
|
|
|
Hearing Issues |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Complete a separate form WC14 for each date of accident) |
|||
|
|
|
|
|
|
|
|||
C. AFFIRMATION OF FILING PARTY
I, [the person whose name appears above], attest and affirm that all information contained herein is true and correct to the best of my knowledge. I understand that knowingly giving false information to obtain or deny workers’ compensation benefits subjects me to civil and criminal penalties.
D. ENTRY OF APPEARANCE
I hereby certify to the existence of a valid fee contract in compliance with Board Rule 108 or a Form
E. CERTIFICATE OF SERVICE
I hereby certify that I have today sent a copy of this form to all of the parties and have sent this form to the State Board of Workers' Compensation, 270 Peachtree St., NW, Atlanta, Georgia
Print Name
Signature
Date
Phone Number
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION 12/2018 |
14 |
NOTICE OF CLAIM |
For injuries occurring on or after July 1, 2007, any claim filed with the Board for which neither medical nor income benefits have been paid shall stand dismissed with prejudice by operation of law if no hearing has been held within five years of the alleged date of injury. (O.C.G.A.
| Fact Name | Details |
|---|---|
| Purpose | The WC-14 form serves as a Notice of Claim for workers' compensation in Georgia, allowing employees to notify the State Board of Workers' Compensation about their claims. |
| Options | Users can check one of three options: Notice of Claim Only, Request Hearing/Notice of Claim, or Request for Mediation/Notice of Claim. |
| Additional Information | If additional employers or insurers need to be added, a new WC-14 form must be completed. Do not alter the existing form; instead, attach extra sheets as necessary. |
| Submission Requirements | The form must be typed or printed in black ink to ensure clarity and compliance with submission standards. |
| Governing Laws | Key governing laws include O.C.G.A. §34-9-18, §34-9-19, and §34-9-100, which outline penalties for false statements and the dismissal of claims after five years without a hearing. |
| Certification | The form includes an affirmation section where the filing party attests to the accuracy of the information provided, acknowledging the potential penalties for false information. |
Form a Corporation in Georgia - Introduces a clear demarcation between amendments requiring member approval and those that do not, reflecting different governance frameworks.
T-200 - The structured format of the form facilitates a straightforward compliance process for solicitors, promoting efficient and timely registration.
Georgia Preliminary Notice of Lien Rights - Georgia's documentation process designed to alert property owners and primary contractors of subcontractors' claims to payments and potential liens on the property.