Fill a Valid Wc 240 Georgia Template
Forms Georgia
Fill a Valid Wc 240 Georgia Template
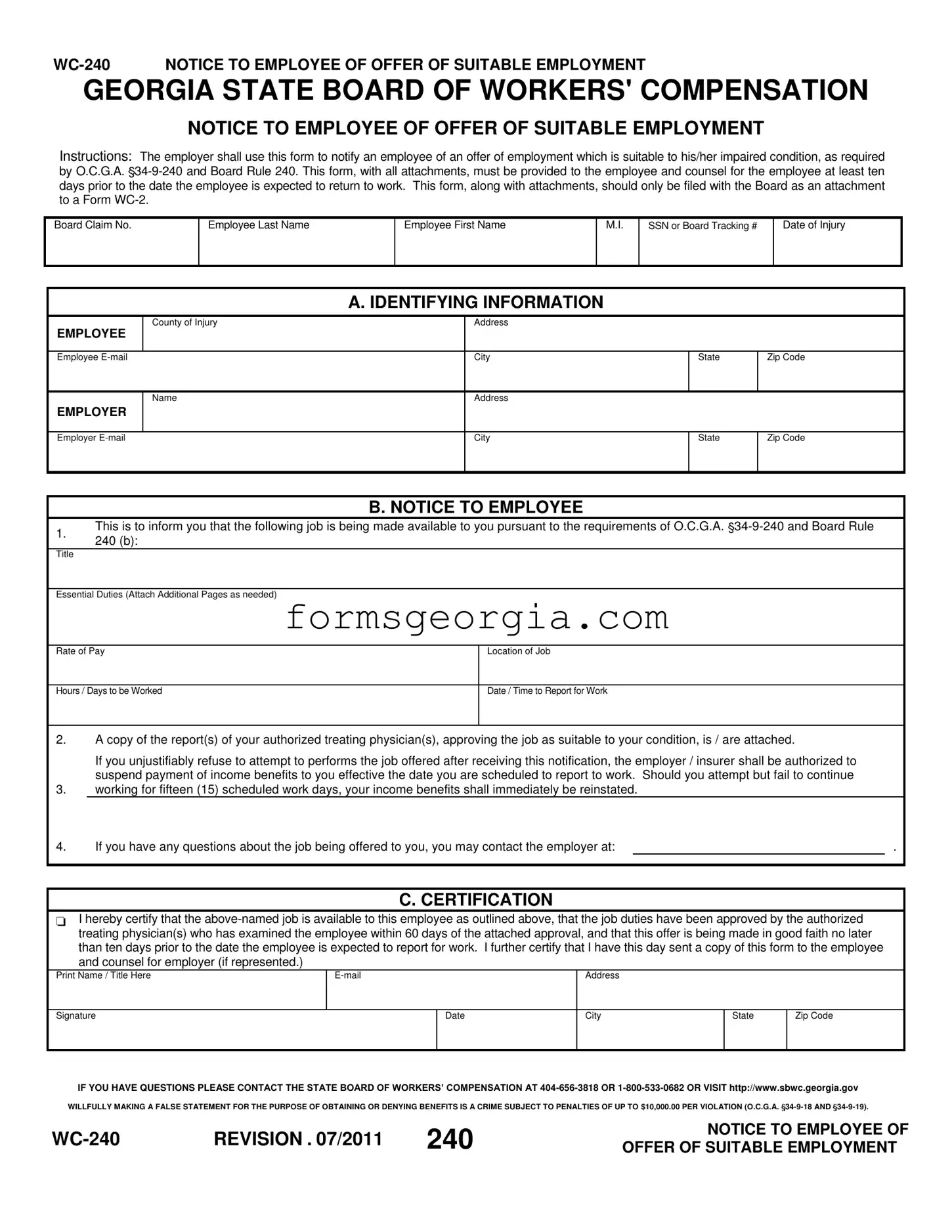
When navigating the complexities of workers' compensation in Georgia, the WC-240 form plays a crucial role in facilitating the return to work for employees recovering from injuries. This form serves as a formal notice from employers to employees, informing them of an available job that aligns with their current capabilities. It is designed to comply with Georgia law, specifically O.C.G.A. 34-9-240 and Board Rule 240. Employers are required to provide this notification at least ten days before the employee is expected to resume work, ensuring adequate time for the employee to assess the offer. The form includes essential details such as the job title, essential duties, rate of pay, location, and the expected hours or days of work. Moreover, it must be accompanied by documentation from the employee's authorized treating physician, confirming that the job is suitable for the employee's condition. Failure to accept a suitable job offer without justification can lead to the suspension of income benefits, emphasizing the importance of this communication. By fostering a transparent dialogue between employers and employees, the WC-240 form helps facilitate a smoother transition back to the workplace while ensuring compliance with state regulations.
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
NOTICE TO EMPLOYEE OF OFFER OF SUITABLE EMPLOYMENT
Instructions: The employer shall use this form to notify an employee of an offer of employment which is suitable to his/her impaired condition, as required by O.C.G.A.
Board Claim No.
Employee Last Name
Employee First Name
M.I.
SSN or Board Tracking #
Date of Injury
A. IDENTIFYING INFORMATION
|
County of Injury |
Address |
|
|
EMPLOYEE |
|
|
|
|
|
|
|
|
|
Employee |
City |
State |
Zip Code |
|
|
|
|
|
|
|
Name |
Address |
|
|
EMPLOYER |
|
|
|
|
|
|
|
|
|
Employer |
City |
State |
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
1.
B. NOTICE TO EMPLOYEE
This is to inform you that the following job is being made available to you pursuant to the requirements of O.C.G.A.
240 (b):
Title
Essential Duties (Attach Additional Pages as needed)
Rate of Pay |
Location of Job |
|
|
Hours / Days to be Worked |
Date / Time to Report for Work |
|
|
2.A copy of the report(s) of your authorized treating physician(s), approving the job as suitable to your condition, is / are attached.
If you unjustifiably refuse to attempt to performs the job offered after receiving this notification, the employer / insurer shall be authorized to suspend payment of income benefits to you effective the date you are scheduled to report to work. Should you attempt but fail to continue
3.working for fifteen (15) scheduled work days, your income benefits shall immediately be reinstated.
4. |
If you have any questions about the job being offered to you, you may contact the employer at: |
|
. |
C. CERTIFICATION
 I hereby certify that the
I hereby certify that the
Print Name / Title Here
Address
Signature
Date
City
State
Zip Code
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION . 07/2011 |
240 |
NOTICE TO EMPLOYEE OF |
|
OFFER OF SUITABLE EMPLOYMENT |
| Fact Name | Description |
|---|---|
| Purpose of Form | The WC-240 form is used by employers in Georgia to notify employees of an offer of suitable employment that aligns with their impaired condition. |
| Governing Laws | This form is governed by O.C.G.A. 34-9-240 and Board Rule 240, which outline the requirements for notifying employees about job offers. |
| Notification Requirement | Employers must provide this form to the employee and their counsel at least ten days before the expected return to work date. |
| Consequences of Refusal | If an employee unjustifiably refuses the job offer after receiving the WC-240, the employer may suspend income benefits starting from the scheduled report date. |
G-7 Return - With detailed sections for tax withheld, tax due, and tax paid, the G-7 form offers a comprehensive framework for tax reporting.
Georgia Nol Carryforward Rules - The form’s inclusion of an “Underestimated tax penalty” section underscores the necessity of accurate tax estimation and payments.